Dr. Jean-Yves Le Goff in Paris
Sleeve / By-Pass Or GPSP
COMPARISON SLEEVE/BYPASS

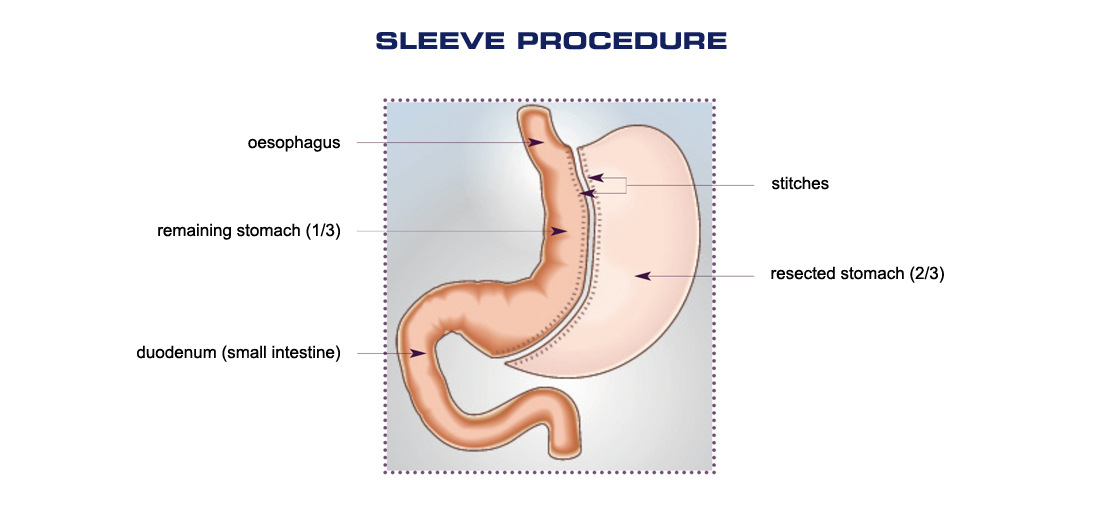
What is sleeve surgery ?
COMPARISON SLEEVE/BYPASS
Gastric sleeve surgery, or sleeve gastrectomy has been carried out for ten or so years in patients with severe obesity and a BMI > 40.
This is a restrictive technique which consists of removing 2/3 of the stomach, and in particular the part containing the cells that secrete the hormone that stimulates the appetite (ghrelin). The stomach is reduced to a vertical tube and the food passes quickly into the intestine. The appetite is also reduced. However, this technique does not hinder the digestion of food.
The operation is irreversible and lasts around 2 hours, requiring 2 to 4 days hospitalisation.
How effective is sleeve surgery ?
The expected weight loss is 45 to 65 % of the excess weight after two years, corresponding to a loss of about 25 to 35 kg.
The main risks of complications are ulcers, leaks, shrinking of the stomach but also post-operative haemorrhage, nutritional deficiencies, inflammation of the oesophagus or dilatation of the stomach.
The estimated mortality is 0.2%.
(Source: Haute autorité de santé, HAS).
It leads to significant mortality: 55 post-operative deaths.
(Source: Haute PMSI 2011)
What is bypass surgery ?
Obesity surgery in Paris
Bypass surgery is the most common obesity surgery and seems to offer the best results in the long term. It has been performed for more than 23 years on patients with a BMI > 45.
This is a restrictive and malabsorptive technique which reduces both the quantity of food intake (the size of the stomach is reduced to a small pouch) and the assimilation of this food by the body, thanks to short-circuiting of part of the stomach and the intestine (no organs are removed).
The operation usually lasts about 1½ to 3 hours and requires 4 to 8 days of hospitalisation.
How effective is bypass surgery ?
The expected weight loss is 70 to 75 % of the excess weight, corresponding to a loss of about 35 to 40 kg.
The main complications encountered are surgical with the formation of ulcers, the appearance of leaks, haemorrhage or shrinking of the junction between the stomach and the intestine. But they may also be functional with hypoglycaemia after meals, constipation or even nutritional deficiencies.
The estimated mortality is 0.5%.
(Source: Haute autorité de santé, HAS).
55 post-operative deaths for bypass surgery in 2011 (PMSI data) and high morbidity (complications) and a very high number of successive repeat operations (up to 8 to 9 times), either due to complications or due to excessive weight gain.

The differences between Sleeve / by-Pass and The Le goff technique
Bariatric Surgery in Paris
The Le Goff Technique (GPSP) is Conservative
Conservative unlike sleeve surgery which consists of ablation of 4/5th of the stomach and bypass surgery which cuts the top of the stomach on which a loop is mounted: this considerably modifies the anatomy and physiology
The Le Goff Technique (GPSP) is Adjustable
Adjustable by inflating the band which reduces the passage of food, increasing satiety, unlike sleeve and bypass surgery which are not adjustable.
The Le Goff Technique (GPSP) is Reversible
Reversible as if the band is removed, the previous anatomy is restored almost identically, unlike sleeve surgery which is irreversible when 4/5th of the stomach is removed, and bypass surgery which is almost irreversible requiring very complex repeat laparoscopic surgery.
The Le Goff Technique (GPSP) is Reproductible
Reproductible car as in the event of complications such as gastric dilatation, another band can be placed above the dilatation. Unlike sleeve and bypass surgery:- Following failed weight loss after sleeve surgery, either an additional sleeve can be done, but usually a bypass is performed of the sleeve so as to add malabsorption to the sleeve.- After failed weight loss following bypass surgery, either ablation of the small stomach is performed if it is dilated, or a band is placed on the dilated stomach to render it modular, or the loop of the small intestine is lengthened to increase malabsorption.
The Le Goff Technique (GPSP) is Non-invasive
Non-invasive as the occurrence of complications is very rare with the Le Goff Technique (GPSP). (All complications total = 2.6%).
Unlike sleeve surgery which causes 6 times more complications (all complications > 12 %) Unlike bypass surgery which causes 12 times more complications (all complications > 25 %)
Fundamentally, complications from sleeve and bypass surgery are far more serious and are often life-threatening.
Remember, mortality is between 0 and 23 years with the Le Goff Technique (GPSP).
Become an actor in your weight loss
the Le Goff Technique (GPSP) in paris
Psychological issues are 80-90 % responsible for severe obesity: about 5 % genetic and 5 % cultural.
Psychological care is essential in helping to treat morbid obesity. Patients need to be looked after and helped to loss the maximum weight. With the Le Goff Technique (GPSP), they are seen more frequently than for sleeve and bypass surgery.
The modularity of the band (inflation and deflation) require the patient to see the surgeon regularly (1 to 3 times in the first year and then at least once a year).
This is the ideal opportunity to see how the band is working in radiology and as “the operation of the band mirrors the psyche”, an interim report can be drawn up on the weight loss and tolerance, and the patient can be directed to a nutritionist if necessary, a psychiatrist-psychoanalyst or a review of sporting practices can be done.
In sleeve and bypass surgery, patients are seen far less often as these are not adjustable techniques, and the consultations required are less frequent. “Forgotten” patients are more numerous for sleeve and bypass surgery than for the Le Goff Technique (GPSP).
The aim of the whole Le Goff team is to make patients actors in their weight loss rather than spectators, which is more the case in sleeve and bypass surgery.
Le goff technique
Bariatric Surgeon in Paris
Indications
The Le Goff Technique (GPSP) is aimed at all obese patients whatever their weight, or BMI. The non-invasive and conservative nature of the Le Goff Technique (GPSP) is essential so as not to add to pre-existing psychological issues problems of deficiencies that exist for sleeve and bypass surgery (more deficiencies for bypass surgery, in vitamin B1-B6-B12-D, Iron, Ca, Mg, Zn and others), and mutilation for sleeve and bypass surgery.
Moreover, the rate of complications with sleeve and bypass is very high quite unlike the Le Goff Technique (GPSP).
Comparison of results
The results of the Le Goff Technique (GPSP) are much better than sleeve and bypass surgery in the long term as:
Psychological care is far greater in the Le Goff Technique (GPSP), as well as the multidisciplinary care.
The Le Goff Technique leads to fewer complications than sleeve and bypass surgery which are invasive, mutilating, quasi-irreversible, non-conservative and non-adjustable techniques, and have a far higher rate of complications.
The Le Goff team remains in constant contact with patients thanks to the inflation and deflation of the band, meaning regular check-ups can be made on weight loss and comfort, unlike the sleeve and bypass surgeries where many patients are lost sight of.
For identical weight loss, the quality of life is far greater with the Le Goff Technique (GPSP) than for sleeve and bypass surgery given the considerable nutritional deficiencies that affect patients’ lives.
An innovative technique
The Le Goff Technique (GPSP) is innovative because:
- it is aimed at all obese patients whatever their BMI
- it is more effective for weight loss over time than sleeve and bypass surgery
- it causes less morbidity unlike sleeve or bypass surgery
- the number of repeat operations is excessively low compared to sleeve and bypass surgery
- it has caused zero mortality for more than 23 years unlike sleeve and bypass surgery
- the quality of life is far higher than with sleeve and bypass surgery (under no circumstances should it be less than the pre-operative situation)
30, Avenue du président wilson Paris 75116